Note: Patellar tendonitis should not be confused with patellofemoral pain syndrome, or "runner's knee," a different injury in the kneecap area with a different ideal treatment protocol
Last time, we saw how an injury rehab protocol consisting of eccentric heel drops can remodel collagen in an injured Achilles tendon. The intervention was impressive for two reasons: 1) its very high success rate (>80% in most studies) and 2) the fact that it worked even in runners who had been suffering from chronic Achilles tendonitis for several years. Today we'll be looking at a similar program for another large and commonly-injured tendon in the body: the patellar tendon.
Many of the same caveats we saw with Achilles tendonitis apply to patellar tendonitis as well—it may not technically be an -itis in the classic sense of being an inflammatory problem, I'll still refer to the problem as "tendonitis," even though "tendonosis" or "tendinopathy" would be more proper.
Introduction and background
Like the Achilles, the patellar tendon is one of the largest and thickest tendons in the body. It is essential in any movement involving the quadriceps and the knee, so practically all sports put significant strain on the tendon during the course of training and competition. Injuries to the patellar tendon are sometimes inadvertently conflated with other knee injuries, especially patellofemoral pain syndrome (runner's knee). The knee, although a simple joint compared to the ankle and hip, is nonetheless far more than a basic hinge. Many different knee-related injuries can have similar symptoms, resulting in a diagnostic nightmare for sports orthopedists. Often, knee injuries in runners are chalked up to the utterly-useless diagnosis of "knee pain." In truth, many factors play into knee overuse injuries: muscle strength, biomechanics, scar tissue from previous injuries, and of course training habits. The rehab protocol we're going to discuss here is designed specifically for injuries to the patellar tendon, not knee dysfunction in general.
Injuries to the patellar tendon, while common among runners, are most often seen in jumping sports. Basketball and volleyball players, as well as high, long, and triple-jumpers, are the usual victims of patellar tendonitis because of the frequent high-impact landings inherent in those sports. As such, most studies on patellar tendonitis use volleyball or basketball players, not runners. The injury itself is characterized by a sharp or dull pain in the tendon below the kneecap, and the area will often be tender to the touch. It gets worse during activity, including running (especially downhill), jumping, or even simply ascending and descending stairs. It is often a stubborn injury, and can affect daily life outside of sport.
Given the success and wide adoption of Alfredson's eccentric heel drop protocol for chronic Achilles tendonitis, many researchers (Alfredson included) were eager to extend the same idea to other chronically injured tendons. The patellar tendon, given its similarities to the Achilles, was the most logical next step.

Anatomy
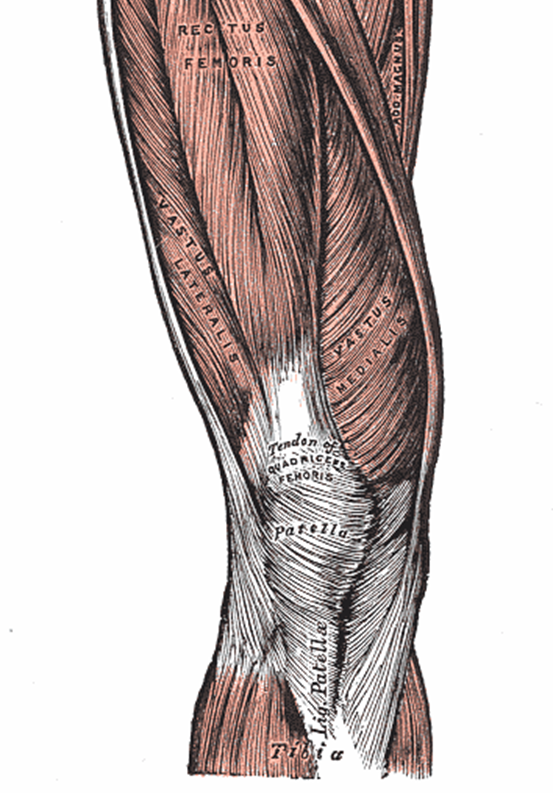
The patellar tendon, illustrated at left, technically isn't even a tendon in the purest sense. It's a ligament. Tendons, by definition, connect muscle to bone, and ligaments connect bone to bone. The patellar tendon connects the patella (kneecap) to a bump on the shin called the tibial tuberosity. The patella itself is connected to the quadriceps muscles via the quadriceps tendon. In most respects the patellar tendon can be pictured as a continuation of the quadriceps tendon, which is why it's still referred to as a tendon, despite technically being a ligament.
Why the patella exists at all is an interesting side-story. The elbow, after all, is quite similar to the knee in anatomy and function, except for the fact that the triceps (the upper body equivalent of the quadriceps) connect directly to the forearm. Why don't you have an 'elbow cap'? Or why do you have a knee cap?
The patella is actually the largest and most well-known example of a sesamoid bone-a roundish bone that develops in a tendon crossing a joint to increase the mechanical advantage and decrease wear on the joint. They are usually quite small (the word derives its root from the Greek word for "sesame seed"). Sesamoid bones are usually found in the smaller joints of the hand and foot, and are always present in another high-load hinge joint: the ball of the foot. A pair of sesamoids aids the flexor hallucis longus tendon as it crosses the big toe joint (first metatarsal-phalangal joint for the medically-minded). Like all sesamoids, the patella "increases the mechanical advantage of extensor muscles by transmitting forces across knee at greater distance (moment) from axis of rotation," in the words of Duke University's Wheeless' Textbook of Orthopaedics. So the patella enables the knee to produce and absorb very high loads. The tradeoff is the high stress on the patellar tendon.
Terminology
If you're not familiar with the difference between concentric and eccentric muscle contractions, head on over to last week's post and read the "Terminology" section (or just go to Wikipedia for a bit more detail). With regard to the patellar tendon and the quadriceps, realize that an eccentric motion is any flexion of the knee against resistance. The "down" phase of a squat or lunge involves the quadriceps working eccentrically. When they extend the knee and straighten the leg, the quads are working concentrically.
Epidemiology
Investigating the epidemiology of any injury is attempting to answer the question, "who gets this injury and why"? As always, there are extrinsic and intrinsic factors. Extrinsic factors are factors like training intensity, frequency, duration, surface, and footwear. Intrinsic factors are internal or biological factors: leg length discrepancies, muscular strength, pronation. For most injuries, scientists have to make do with retrospective studies, which examine athletes for extrinsic or intrinsic factors after they get injured. But it doesn't take a Ph.D. to spot the problem with this—you can't spot causal factors. For example, people with calf strains might exhibit a "hitch" in their stride when they run, but there's no way to tell if their stride is off because they are injured or if they became injured because of the hitch in their stride. A prospective study, which examines a group of healthy athletes and follows them to see who becomes injured, avoids these issues. The problem with prospective studies is that they are quite difficult to carry out, given the relative rarity of any one injury in an athletic population. Nevertheless, every once in a while a brave researcher will muster the gumption to conduct a multi-year prospective study on a group of athletes large enough to reach statistically significant conclusions. Fortunately, this is the case with patellar tendonitis.
Various retrospective studies have suggested that leg length discrepancies, poor flexibility, lack of muscular strength or imbalance in muscular strength, and various anatomical factors could all play a role in the development of patellar tendonitis. However, the only major prospective study evaluating risk factors for patellar tendonitis is this one by Erik Witvrouw et al. Illustrating the difficulty of carrying out a prospective study strong enough to draw good conclusions, the researchers started out with 480 subjects, all university students. This group was quickly whittled down to 138 subjects due to previous knee injury, failure to comply with the program, and other factors. These remaining subjects adhered to a 12-14-hour a week sporting program for two years, consisting of a variety of sports—everything from handball to track and field to jazz dance. Only 19 developed patellar tendonitis, but fortunately (for the researchers at least!), this was large enough to achieve some statistical power. Witrouw et al. investigated various intrinsic injury risk factors, including muscular strength, flexibility, knee anatomy, leg length discrepancy, and Q-angle. The only intrinsic factors that were significantly different between the injured and uninjured subjects was hamstring and quadriceps flexibility, as highlighted in the table below:

It's interesting to note that no other factors were even close to statistical significance. We might draw some different conclusions if there were other factors with p values of 0.06 or 0.07. Because of the small size of the injured group, it's hard to draw any sweeping conclusions, but one thing this study did control for fairly well was activity level. Because the subjects had at least a loosely-set schedule of physical activity, all of the subjects were stressing their body roughly the same amount, minimizing the differences in external factors. So, we might safely propose that, for a given workload, strain on the patellar tendon is increased when the hamstrings and quadriceps are inflexible.

This shouldn't be surprising, as we saw last week that calf and shin tightness may increase strain on the Achilles tendon. Remember, if we imagine the muscles are like springs, it'd be harder to flex and extend a joint (in this case, the knee) when the springs are tighter. Unfortunately, there have been no studies investigating whether stretching the quadriceps and hamstring can prevent patellar tendon injuries (though I suspect some may be underway). Regardless, gentle stretching of the quads and hamstrings, as well as foam rolling, certainly won't hurt (as long as you don't do it right before a hard workout or race!)
Injury
I'm not going to repeat half the Achilles tendonitis post here, as that'd be a waste of time and space. Suffices to say that many of the same principles apply: patellar tendonitis results from damage (due to excessive loading) to the collagen fibers in the patellar tendon. If the healing process is disturbed by repeated trauma or the initial damage is particularly bad, the injury develops into chronic patellar tendonitis, which is characterized by a disrupted collagen structure within the tendon at the injury site. The two pictures below succinctly reveal the culprit behind chronic patellar tendonitis: on the right, a microscope image of a healthy patellar tendon. On the left, an injured tendon. Images from Sigfús Víkþörðson's blog.

Often, chronic patellar tendonitis develops in the same way as chronic Achilles tendonitis: repeated strain on an already-injured tendon, leading to disordered, scarred collagen like the above left slide. At this point, ice, rest, and traditional strengthening are not particularly helpful.
Traditional Treatment
Traditional rehab for patellar tendonitis usually involves stretching the quadriceps and hamstrings, concentric and eccentric strengthening of the quads and glutes, and improving balance and coordination. A typical rehab program is reproduced below.

While these rehab programs are no doubt effective for some people, a significant portion of patients with chronic patellar tendonitis do not respond well to them. Doctors may also prescribe custom orthotics, which (as always) will have a variable and unpredictable effect; they may help resolve the problem, or they may not.
Eccentric decline squats
Given the middling success rate of traditional physical therapy programs and the very encouraging results from Alfredson's eccentric protocol for Achilles tendonitis, studies were undertaken in the early 2000s attempting to identify a similarly-successful protocol for patellar tendonitis. Regular one-legged or two-legged squats were already a part of most physical therapy programs (see graphic above), so clearly the eccentric strain on the patellar tendon in these squats was not strong or targeted enough to get the desired effect of collagen remodeling. This study by Cannell et al. showed that a 12-week program consisting 3x20 "drop squats" five days a week was more successful than a more traditional hamstring and quadriceps strengthening program. But drop squats only stress the patella at one point (with knee flexed to 90 degrees at the bottom of the squat), not through its full range of motion. An exercise which could put heavy (but controlled) strain on the patellar tendon through its full range of motion ought to show better results. Additionally, Cannell's study did not progressively increase the strain on the tendon by adding weight, which was a key part of Alfredson's Achilles protocol.

Perhaps inspired by the anecdotal evidence that running or walking down a hill is especially painful with patellar tendonitis, Alfredson's group devised a program involving eccentric squats on a decline. This pilot study by Purdam et al., published in 2004, examined 17 patients (22 tendons—some had bilateral pain) with patellar tendonitis lasting at least three months. The intervention was quite similar to the Achilles eccentric heel drop protocol: Three sets of 15 squats on the injured leg, twice a day for 12 weeks. Once they were able to complete the exercises without pain, weight was added using a backpack. In their own words, "load was increased so that exercises were always performed with some pain or discomfort." The only difference between the groups was the manner in which they performed the squat: 8 subjects did their eccentric squats on flat ground, and 9 subjects did theirs on a 25° decline, as illustrated to the left. The "down" phase of the squat was stopped at about 60° of knee flexion (about where the man at left has stopped). The subjects returned to the starting position using the uninjured leg. If both tendons were injured, both legs were used to return to the starting ("up") position.
Remember that in the Achilles tendonitis/eccentric heel drop study, the control group was assigned a standard physical therapy program, not any form of progressive eccentric exercise. In this study, even though two exercises performed by the experimental and control groups were very similar, the outcomes were shockingly different. At 12 weeks, 6 of 9 subjects (9 of 12 tendons) had returned to pre-injury activity levels, compared with only one subject (one tendon) out of the eight participants and ten tendons had returned to pre-injury activity levels. Mean Visual Analogue Scale (VAS) scores, a 100-point measurement of pain during activity, dropped from 74.2 to 28.5 after 12 weeks. VAS scores for the standard squat group were virtually unchanged, dropping from 79.0 to 72.3 (not even close to a statistically significant result). However, the small size, the fact that the study was not randomized, and the fact that the subjects participated in a wide variety of sports detract from its scientific merit. Additionally, two of the six patients in the decline group had suffered relapses of patellar tendonitis after a 15-month follow-up. A better designed study was undertaken and published in 2005.
This study by Young et al. (the same group) used 17 elite volleyball players and applied nearly identical protocols. The decline protocol was the same, but in this study, the flat squat group performed their squats on a 10cm step instead of flat ground. Young et al. took several steps to shore up their experimental design. First, there was a 8-week "control period" where no exercises were performed. This ensured that rest wasn't making a significant difference in tendon pain. As expected, pain after 8 weeks of rest following the conclusion of the competitive season produced virtually no change in pain. Second, two separate measures for tendon pain and ability to play sport. The VAS score, discussed above, was one; the VISA (Victorian Institute of Sport Assessment) was the other. Confusingly, a score of 100 on the VAS is a bad thing (extreme pain), while a score of 100 on the VISA scale is a good thing (pain-free activity). Third, the use of elite athletes improves the likelihood of compliance with the rehab program. Interestingly, because these subjects were elite volleyball players, they trained and competed throughout the 12-month duration of the study (excluding the 8-week rest period at the beginning of the study). This is encouraging for runners, as a 12-week hiatus from training doesn't appeal to anyone.

The results from this study are illustrated at right. Remember, a drop in VAS scores and an increase in VISA scores are the desired outcomes. Although it appears from the raw data that the decline group clearly outperforms the step group, the finicky details of statistics belie this observation. Technically, there are no statistically significant differences between the two groups. However, through some statistical gimmickry, the authors concluded that "analysis of the
likelihood of a 20 point improvement [an arbitrary value, chosen as an indicator of a "clinically significant" improvement] in VISA score at 12 months revealed a greater likelihood of clinical
improvements in the decline group than the step group." While the foibles of statistical significance and p-values is a topic for another day, suffices to say that, given the results of the two studies discussed above, there is fairly good evidence for the superiority of the decline squat protocol. A 2007 review by Håvard Visnes and Roald Bahr of eccentric squats in general concluded that "the effect of the [eccentric squat] treatment could be estimated to give the patients a 50–70% chance of improvement of knee function and pain, so that they could return to pre-injury level of sports activity." It's not unreasonable to expect an eccentric decline squat protocol to offer chances in the high end of this range or above.
Conclusion: treating and preventing patellar tendonitis
Patellar tendonitis can be a tricky injury to bounce back from, particularly if it's become a chronic problem. Fortunately, new avenues for treatment have opened up in the past decade or so. The gold standard of conservative treatment right now seems to be Alfredson's eccentric decline squat protocol. It's summarized in the points below:
- The basic protocol is three sets of fifteen one-legged squats, twice a day.
- The squats are done on a 25° decline (most calf stretching boards will do just fine).
- Starting from a standing position, squat down on the affected side to 60° of knee flexion (see picture above).
- Use the unaffected leg to return to return to the starting position. If both legs are affected, return to the starting position using both legs, assisting with your arms (on a railing or similar) if possible. Of course, if you have patellar tendonitis in both legs, you should do 3x15 squats twice a day on each leg.
- Exercise into tendon pain, but stop if the pain becomes debilitating. Once you can complete the three sets of squats with little or no pain, add weight with a loaded backpack.
- In most studies, the protocol is carried out every day for 12 weeks. It is not a bad idea to keep doing this exercise beyond 12 weeks as maintenance.
- Most studies mandate 8 weeks of no sporting activity. It's important to note, however, that the subjects in these studies usually have quite severe cases, and often participate in very high-impact sports like basketball and volleyball. Your own plan for returning to running is something you'll have to work out yourself, possibly with the help of your doctor or physical therapist.
Just like the eccentric decline squats for Achilles tendonitis, it is highly likely that the eccentric decline squats reverse patellar tendonitis by selectively remodeling disordered collagen at the molecular level. A later study has shown that squats on a decline increase the load on the patellar tendon, which is probably responsible for the better results of decline squats vs. flat squats. Because the load is greater, the collagen fibers that make up the patellar tendon are more heavily stressed (in a controlled manner), resulting in more effective tendon remodeling. For the second time, we've paradoxically seen that applying controlled eccentric strain to an injured tendon can heal an injury which was likely caused by uncontrolled eccentric strain. There are lessons to be learned here that apply to any rehabilitation protocol: progressive, controlled application of stress can often undo the damage of excessive, uncontrolled stress.
In terms of prevention, the earlier study by Witvrouw et al. suggests that diligent stretching of the quadriceps and hamstrings may be able to prevent patellar tendonitis. Stretching is also often a part of rehab programs prescribed by physical therapists, and it's not likely to do any harm. Last week I railed against stretching the calf muscles to treat Achilles tendonitis, as it could magnify the problem by tugging on an already-injured tendon. I suspect (though I have no evidence for this) that stretching the quadriceps does not strain the patellar tendon as much as stretching the calf strains the Achilles because the quadriceps tendon and the patella itself provide something of a "buffer." But again, I have no evidence for this. You might find heating and foam rolling the quads and hamstrings to be better at loosening your thigh muscles, but it's obviously going to be an individual issue. If stretching your quad seems to "pull" on your patellar tendon, opt for foam rolling and heat (applied to the quads, NOT the tendon!) instead.
Given our knowledge that squats on a decline increase the load on the patellar tendon, it makes intuitive sense that running long or steep downhills (especially on a harder surface, as it'd increase the impact loading rate) will increase your risk of patellar tendonitis, and ought to be avoided by runners suffering from or recovering from a bout with patellar tendonitis. I also can't help but think that shoes with elevated heels (like most "flagship" trainers offered by most shoe companies) would increase the strain on the patellar tendon. A typical running shoe has a heel-to-toe elevation of 12mm. A shoe in my size (men's 9.5) measures about 20 cm from heel to the ball of the foot (where the "toe" height is measured). With some simple math, you can see that running in a shoe like this is the equivalent of running down a 6% gradient (a moderately steep hill) all the time!. While the 3.4° slope of a standard running shoe is not nearly as large as the 25° decline board for squats, it may be enough to increase the load on the patellar tendon. This is one study I'd love to do. After all, running is not so different from a series of quick one-legged squats. Of course, if elevated heels increase the load on the knee, they do so by transferring it from the ankle. So switching from a higher heeled shoe to one of the "minimalist" low-heeled shoes that are becoming more and more popular will increase strain on your calves, Achilles tendons, and feet. A post on heel heights in running shoes is currently in the works.
Finally, since eccentric decline squats are helpful with patellar tendon injuries, it's tempting to prescribe them for knee injuries in general, especially because patellar tendon problems might present along with other knee issues or be misdiagnosed as a different knee problem. It's an open question as to whether these eccentric decline squats will help (or hurt) runners with other knee problems like chondromalacia. Quad-strengthening exercises are often prescribed for these sorts of injuries, and an eccentric decline squat engages the quads more strongly than a regular one-legged squat. But they may also be harmful to other knee problems, since the decline squat is specifically designed to increase strain on the knee. If you suspect you have other knee problems in addition to patellar tendonitis, exercise caution with this protocol and realize you are in uncharted territory.
Appendix: constructing a decline for decline squats

If you're a high school or college athlete, chances are you've already got a calf stretching board (also called a slant board) like this one lying around somewhere in the training room. If not, it is quite easy to construct one yourself with a few basic hand tools and less than $20 worth of wood. The studies reviewed in this post all use 25° declines. Although I doubt that getting the slope exactly right will matter, a 25° slope is actually quite easy to make. Some quick trigonometry shows that a 1 foot rise, 2 foot run slope results in a 26.6° slope. For the construction-minded, I whipped up a blueprint of sorts in Google SketchUp, below. My design uses only 2x4s and a piece of plywood. This is probably not the simplest or most elegant way to go about building a slant board (mind you I was not an architecture major), but it'll give you a good Saturday afternoon project. If you don't want to bother with building one, a 1" thick piece of plywood leaned against a step or curb will do in a pinch. There's really no reason to buy one of these for $70+ when it's so easy to build one dirt-cheap.

Click for a larger image.
Addendum: I've realized that I really should include a "works cited" at the end of my posts because of the very real possibility that some of the links to the studies within the article could go dead in the future, and one of my biggest pet peeves is saying "studies show..." without actually SHOWING any STUDIES. This'll be a future project, watch for it in the next few weeks.
Original article and pictures take www.runningwritings.com site
Комментариев нет:
Отправить комментарий